Other Common Problems We Treat:
Laser Treatment for Toenail Fungus
Warts, Laser Treatment of Plantar Warts, (Verruca)
Bunion: Diagnosis, Treatment and Surgery
Bunion with Stiff & Painful Joint (Hallux Rigidus)
Hammertoe
Neuroma: Diagnosis & Surgery
Ingrown Toenail Treatment
Tailor’s Bunion
Bone Spurs
Gout
Can’t Find What You’re Looking For? Give Us A Call!
Bone Spurs
Bone spurs can develop almost anywhere on the foot. They are often a reaction to pressure or a result of an arthritic change near a joint. The term “bone spur” is often used to describe multiple types of foot problems. The term “calcium deposit” is sometimes used to describe a bone spur.
Heel Spur
A heel spur is a horizontal projection of bone growth, extending forward from the bottom of the calcaneus or heel bone. It can be quite painful, and is often associated with plantar fasciitis. They can exist on one or both heels, and take many years to develop. Even though this type of spur can be present for a long time, it may not be painful until it reaches a certain size. The diagnosis is made from a lateral view x-ray of the foot.
Toe Spur
Bone spurs around the toes are often present around the bunion joint (1st metatarsophanageal joint) or within the toes themselves. In the front part (the forefoot) spurs are often associated with a corn or callous. The medical terminology for a corn or callous is a hyperkeratosis. These types of spurs can often be felt through the skin, and are also visible on x-ray. Toe bone spurs can be painful with shoe pressure.
Treatment choices range from conservative to more aggressive surgical options. Initially, trimming the corn or callous on the skin can be effective. However, since the skin problem is actually caused by the underlying spur, bony smoothing of the spur usually cures this type of problem.
Arch Spur
An irritation can develop on the top of the foot in the area of the arch. This area becomes painful when the shoe laces are tied or with pressure from a slip-on shoe. Examination of this area often shows redness of the skin and hardness beneath the skin. This is associated with a spur or overgrowth of bone in the midfoot area. The most common location is at the joint between the first metatarsal and the first cuneiform bones. The spur development is associated with arthritis in the area.
The treatment of this problem often requires surgery. The excessive build-up of bone needs to be removed by smoothing or filing the enlargement.
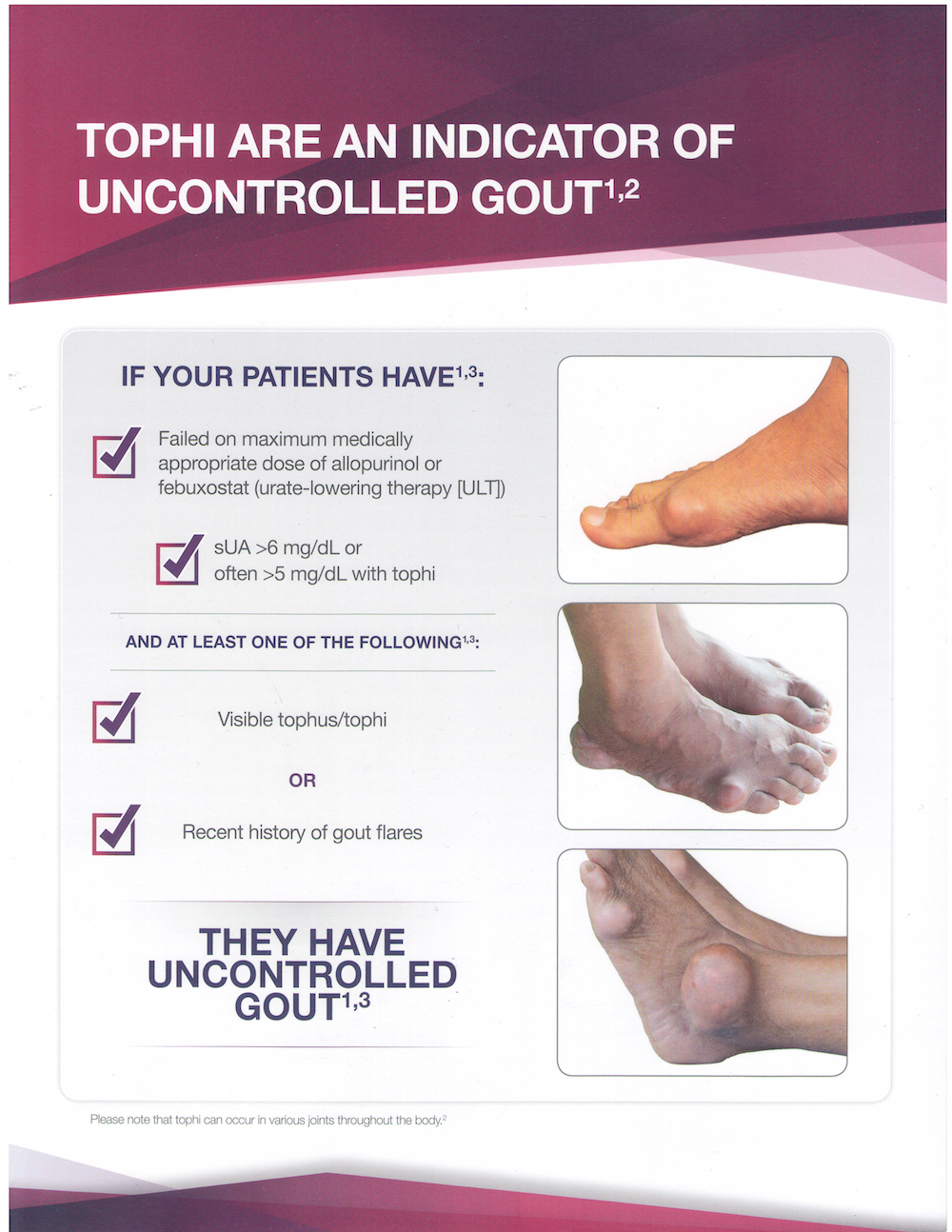
Gout
Gout is a metabolic disorder that results from the build-up of uric acid in the tissues or a joint, most often the big toe joint. An acute attack of gout can be very painful, marked by intense pain that comes on suddenly, redness, swelling, and warmth over the joint. The increased warmth over the joint is most noteable. Even light pressure, such as bedsheets, can cause remarkable pain. Gout usually only affects one joint at a time. Usually there is no history of trauma.
Gout attacks are caused by deposits of crystallized uric acid in the joint. Uric acid is normally present in the blood and eliminated in the urine, but in people who have gout, abnormally high amounts of uric acid accumulates and crystallizes in the joints. Uric acid is the result of the breakdown of purines, a protein that is found naturally in our bodies and in food.
Gout occurs most commonly in the big toe because uric acid is sensitive to temperature changes. At cooler temperatures, uric acid turns into crystals. Since the foot is furthest from the heart, it’s the coolest part of the body. However, gout can affect any joint in the body.
The tendency to accumulate uric acid is often inherited. Other factors that put a person at risk for developing gout include: high blood pressure, diabetes, obesity, surgery, chemotherapy, stress, and certain medications and vitamins. For example, the body’s ability to remove uric acid can be negatively affected by taking aspirin, some diuretic medications or water pills, and the vitamin niacin. While gout is more common in men aged 40 to 60 years, it can occur in younger men and also occurs in post-menopausal women.
Consuming foods and beverages that contain high levels of purines can trigger an attack of gout. You may be able to reduce your chances of getting a gout attack by limiting or avoiding the following foods and beverages: shellfish, organ meats (kidney, liver, etc.), red wine, beer, and red meat.
Examination, blood tests (for excessive uric acid) and x-rays are used to determine the diagnosis. Microscopic examination of a sample of the joint fluid, looking for uric acid crystals, provides the most accurate diagnosis.
Initial treatment of an attack of gout may include the following:
Medications: Prescription medications are used to treat the pain, swelling, and inflammation.
Dietary restrictions: Foods and beverages that are high in purines should be avoided, since they are converted to uric acid in the body.
Fluids: Drink plenty of water and other fluids each day, while also avoiding alcoholic beverages, which cause dehydration.
Elevate the foot: Avoid standing and walking to give your foot a rest. Elevate your foot level with or slightly above the heart to help reduce the swelling.
The symptoms of acute gout and the inflammatory process usually resolve in three to ten days with treatment. Medications are available that will limit the excessive production of uric acid.
Repeated gouty attacks can cause gouty arthritis within big toe joint. This type of arthritis often causes erosions or destruction of the surfaces of the joint. Surgery may be required to remove the uric acid crystals and repair the joint.